
What you need to know
Healthcare in the United States operates as a collection of state-based systems layered on top of federal programs. Where someone lives can shape what insurance they have access to, how much they pay for it, and what care they receive. In this brief, we:
- Explain how federalism shapes health care policy
- Describe how acts of Congress reinforce state control over healthcare
- Examine how these variables affect access, cost, and care
What level of control do states have over healthcare?
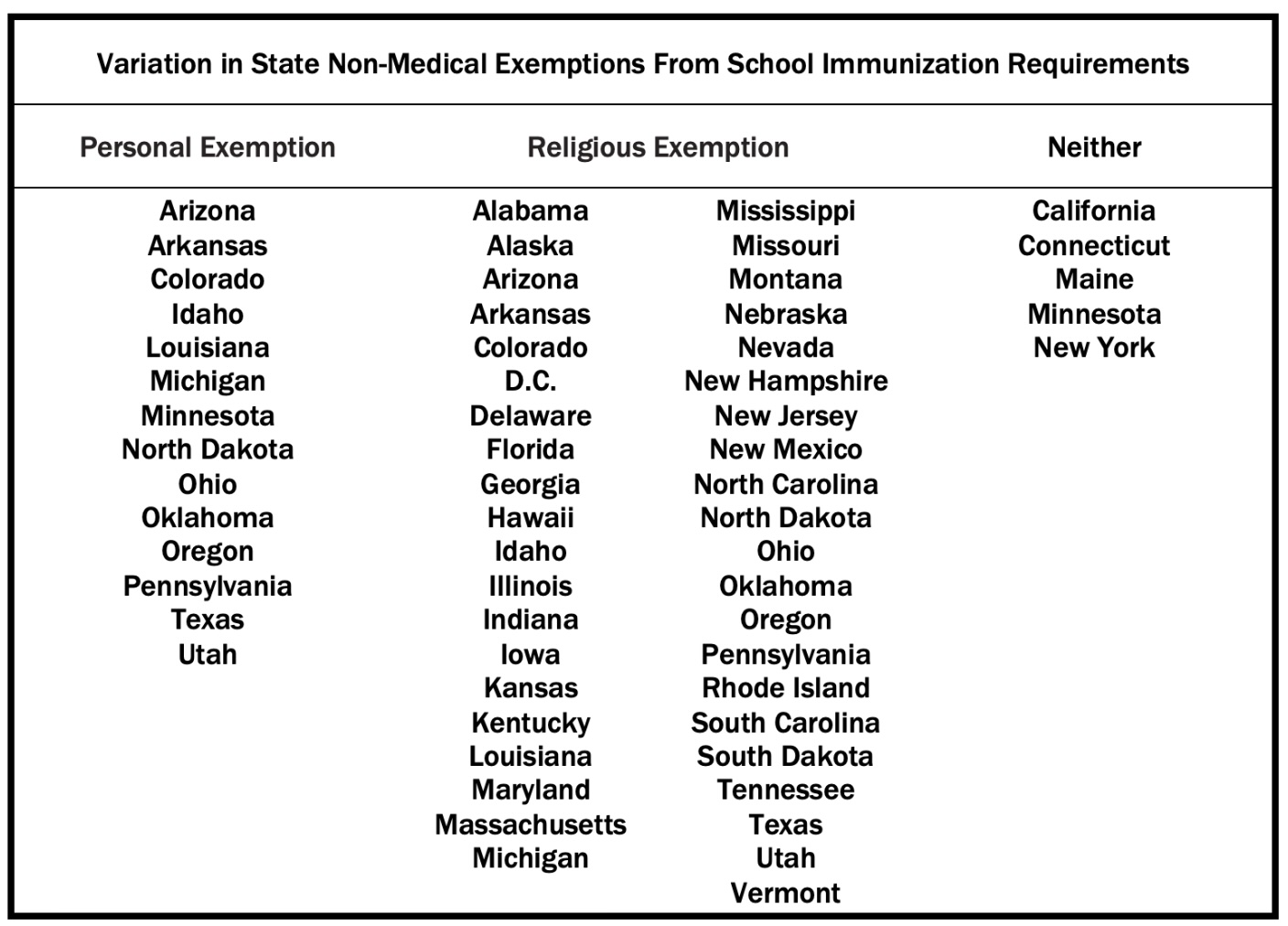
The variation in healthcare and health policies across states is largely a product of federalism, the division of power between the federal government and the states. Under the U.S. Constitution, states retain broad authority over public health and safety. Their powers include permitting or banning certain procedures or strategies of care, licensing doctors, regulating hospitals, deciding if children must be vaccinated to attend school, overseeing insurance markets, and more. The table below describes which states allow parents to opt out of vaccines for their children attending public school in those states.
The federal government plays a major role through programs such as Medicare and Medicaid and through national laws such as the Affordable Care Act (ACA). But federal health care laws are written with a degree of flexibility so that state governments can decide how to implement them. States are the level of government that regulate provider licensing and scope of practice (for example, what care nurse practitioners or physician assistants can provide), as well as rules for insurance marketplaces, and decide whether they expanded Medicaid under the ACA.
What did the McCarran-Ferguson Act do?
In 1945, Congress passed the McCarran-Ferguson Act, which formally gave states the authority to regulate insurance. This action followed the Supreme Court's ruling in United States v. South-Eastern Underwriters Association (1944) that the federal government could regulate insurance under the Commerce Clause. Instead of expanding federal control, Congress chose to reinforce state authority.
The McCarran-Ferguson Act created exemptions for health insurance companies from federal antitrust rules. Critics argue that this exemption has reduced competition and contributed to higher premiums. In contrast, supporters argue that it helped stabilize early insurance markets in the 1940s as employer-based insurance became the norm.
Efforts to roll back this exemption have received bipartisan support over time, including legislation such as the Competitive Health Insurance Reform Act of 2017, which passed the House 416-7 but was never taken up in the Senate. A similar bill passed the House in 2010 with a 406-19 vote, but wasn’t voted on in the Senate.
What are the consequences of state variation in healthcare?
Owing to the McCarran-Ferguson Act and subsequent laws, insurance companies must follow state-specific rules, which means that plans are approved at the state level and states permit different types of coverage or reimbursement. For example, some states require that insurers cover fertility treatments, while others do not. Additionally, consumers generally cannot purchase plans across state lines.
Depending on state policy decisions, Medicaid eligibility rules, insurance premiums, out-of-pocket expenses, and hospital pricing rules differ. In addition, public health programs like mental health and maternal care are funded at different levels across states.
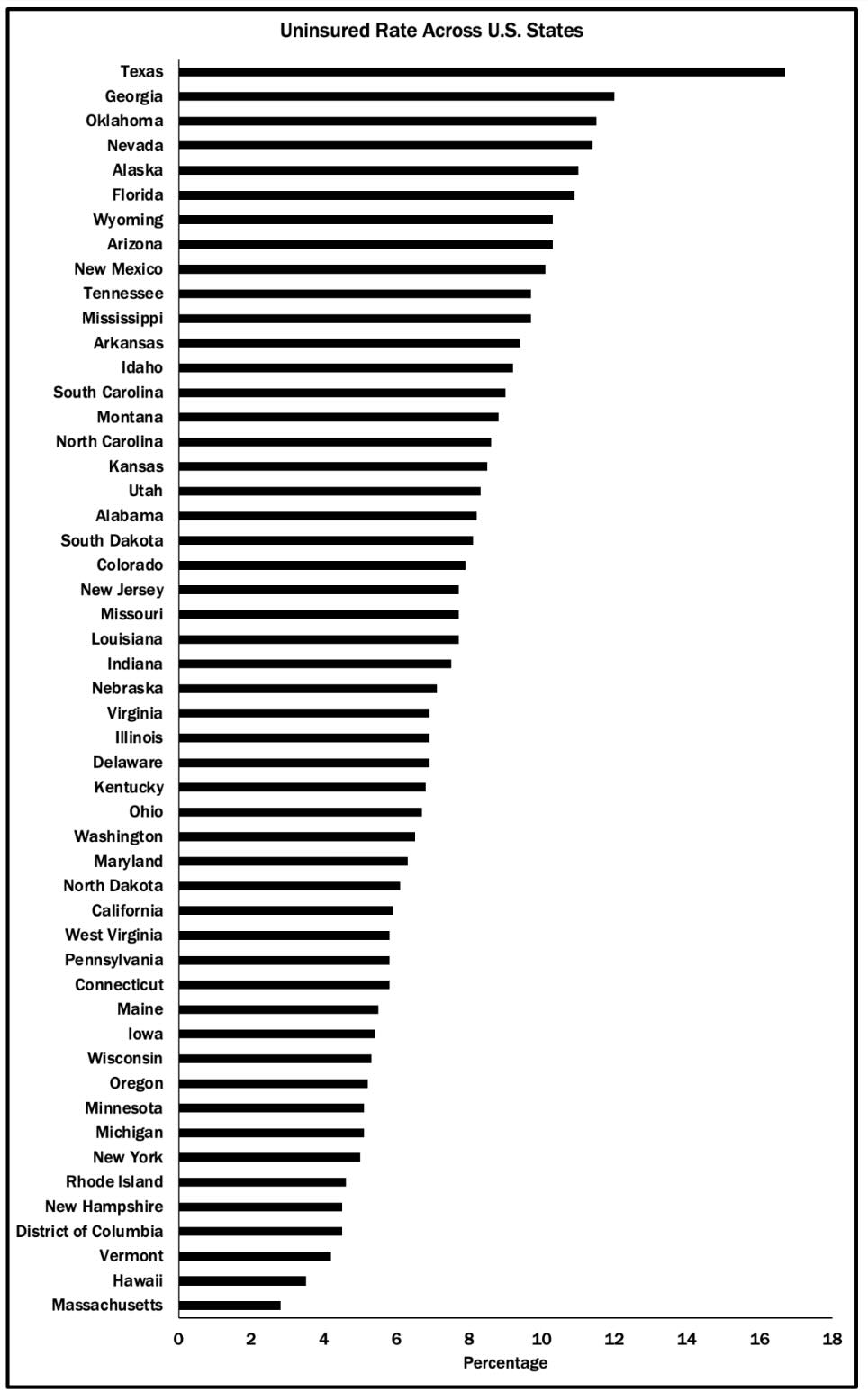
One way to easily grasp how different states are regarding healthcare is to look at variation in the uninsured population, although this variation is the product of differences in demographics, socio-economic status, personal preferences, and state regulations.
On a more practical level, the dominance of state-level regulation of healthcare means that Americans' options for care are often limited to the providers (doctors, laboratories, facilities, etc.) within their state of residency. It is often more expensive, or even impossible, to have insurance pay for care from providers in other states, or to purchase health insurance from a company not licensed in the state where an individual resides. All of these limitations rest on the decision made in the McCarran-Ferguson Act and reinforced by subsequent legislation.
The Takeaway
Healthcare varies by state because federalism and laws enacted by Congress give states primary authority over insurance and care, leading to real differences in access, cost, and quality.
It would be possible to regulate healthcare at the national level, however, doing so would require a combination of congressional action, executive orders, and, perhaps, amendments to the Constitution.
Enjoying this content? Support our mission through financial support.
Further reading
Tolbert, J., Diana, A., Mudumala, A., Brooks, T., Yafimenka, Y., & Lin, A. (2026). An Early Look at Policy Decisions as States Get Ready to Implement Work Requirements. KFF. https://tinyurl.com/52ecud3x, accessed 05/11/26.
HealthCare.gov. (2018). How insurance companies set health premiums. https://tinyurl.com/4fstbw9h, accessed 05/11/26.
Sources
U.S. House of Representatives. (1945). Act of March 9, 1945. Govinfo.gov. https://tinyurl.com/2s472yk8, accessed 05/11/26.
KFF. (2025). Mandated Coverage of Infertility Treatment. https://tinyurl.com/3ksuszam, accessed 05/11/26.
CNN. (2026). House votes to kill antitrust exemption for health insurers. https://tinyurl.com/45ssh838, accessed 05/11/26.
U.S. House of Representatives. (2017). H.R. 372 - Competitive Health Insurance Reform Act of 2017. Congress.gov. https://tinyurl.com/44re7257, accessed 05/11/26.
National Conference of State Legislatures. (2026). State Non-Medical Exemptions From School Immunization Requirements. https://tinyurl.com/58j5ru38, accessed 05/11/26.
Contributors
Lindsey Cormack (Content Lead) is an Associate Professor of Political Science at Stevens Institute of Technology and the Director of DCinbox, a comprehensive digital archive of Congress-to-constituent e-newsletters. She received her PhD from New York University. Her research explores congressional communication, civic education, and electoral systems. Lindsey is the author of How to Raise a Citizen (And Why It’s Up to You to Do It) and Congress and U.S. Veterans: From the GI Bill to the VA Crisis. Her work has been featured in The New York Times, The Washington Post, Bloomberg Businessweek, Big Think, and more. With a drive for connecting academic insights to real-world challenges, she collaborates with schools, communities, and parent groups to enhance civic participation and understanding.
William Bianco (Research Director) is Professor of Political Science at Indiana University and Founding Director of the Indiana Political Analytics Workshop. He received his PhD from the University of Rochester. His teaching focuses on first-year students and the Introduction to American Government class, emphasizing quantitative literacy. He is the co-author of American Politics Today, an introductory textbook published by W. W. Norton, now in its 8th edition, and authored a second textbook, American Politics: Strategy and Choice. His research program is on American politics, including Trust: Representatives and Constituents and numerous articles. He was also the PI or Co-PI for seven National Science Foundation grants and a current grant from the Russell Sage Foundation on the sources of inequalities in federal COVID assistance programs. His op-eds have been published in The Washington Post, Indianapolis Star, Newsday, and other venues.




